 Home
Home Archive
Archive Search
Search Sign In
Sign In Site Menu
Site Menu


This Article

Citations
 CrossRef (0)
CrossRef (0) - Google Scholar
-
Scopus (0)

Except where otherwise noted, this work is licensed under Creative Commons Attribution-NonCommercial 4.0 International License.
Cardiac Magnetic Resonance Imaging Findings in a Patient with Ebstein’s Anomaly and Left Ventricular Dysfunction
Abstract
Ebstein anomaly is characterized by apical displacement of the septal and posterior tricuspid valve leaflets, leading to atrialization of the right ventricle and could be diagnosed in a routine transthoracic echocardiography exam. We reported a young man with right sided heart failure symptoms who was found to have biventricular failure with suspected apical displacement of septal leaflet of tricuspid valve. For better evaluation, cardiac magnetic resonance imaging (CMR) was performed and nicely proved the diagnosis of Ebstein's anomaly with late intramyocardial enhancement of both left and right ventricles. CMR has the potential for providing information while echocardiography cannot, especially regarding the right ventricle and related myocardial problems, and Ebstein’s anomaly with decreased left ventricular (LV) systolic function.
Keywords: Ebstein’s Anomaly; Heart Failure; Magnetic Resonance Imaging
1. Introduction
Ebstein anomaly is characterized by apical displacement of the septal and posterior tricuspid valve leaflets, leading to atrialization of the right ventricle and could be diagnosed in a routine transthoracic echocardiography exam.
2. Case Presentation
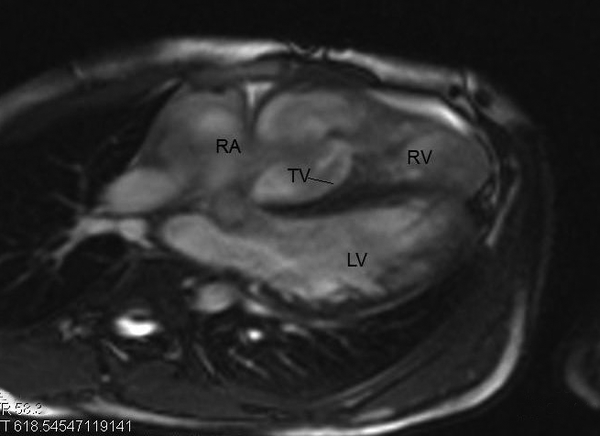
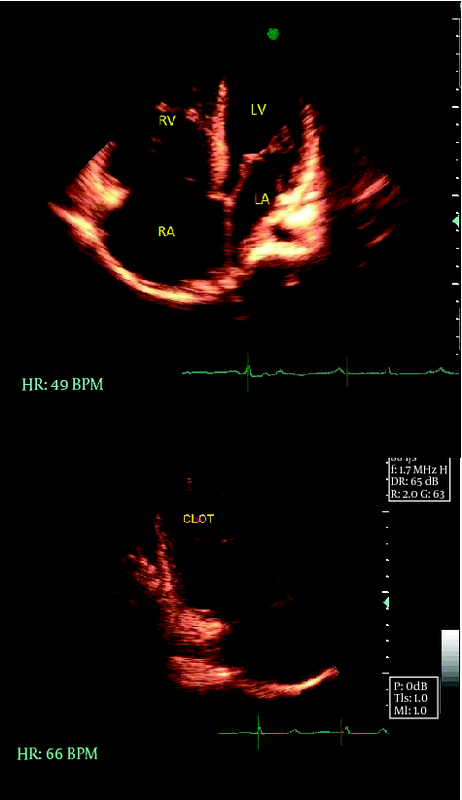
A 26 year old man with a two-month history of fatigue and shortness of breath referred to heart failure clinic. On physical examination, he had jugular venous distension, prominent apical impulse and a soft 2/6 systolic murmur at apex. Trans-thoracic echocardiography demonstrated mild LV enlargement with severe LV systolic dysfunction (EF = 20%), left atrial (LA) enlargement and mild to moderate mitral regurgitation (MR). There was also severe right ventricular (RV) and right atrial (RA) enlargement and severe RV dysfunction, a marked smoke pattern in both RA and RV and a malcoapted tricuspid valve but no detectable TR in color flow Doppler study. A large mass, most probably a thrombus was obvious in RV apex (Figure1a-b). Findings were in favour of a biventricular failure with prominent RV involvement, yet a diagnosis of Ebstein’s anomaly was also suspected regarding the apparent apical displacement of septal leaflet of tricuspid valve with some tethering of anterior tricuspid leaflet. CMR examination was done on a 1.5 T scanner (Siemens Avento) and Gadolinium-DTPA 0.2 mmol/kg was administered intravenously and delayed enhancement short axis and long axis images were recorded 10-15 min later. Displacement of thickened septal tricuspid valve leaflet toward RV was found and confirmed Ebstein’s anomally (Figure 2). Both ventricles showed severe systolic dysfunction. An extensive intramyocardial hyperenhancement of left ventricle with sparing of sub endocardium (nonrelated to a coronary artery territory) was demonstrated (Figures 3,4). In addition, hyper enhancement of right ventricle, right atrium and inter atrial wall was also shown. There was a clot in right ventricle in delayed enhancement sequence (Figures 5).

|
Figure 1.
RV Apex, a) Echocardiography revealed biventricular enlargement and systolic dysfunction, b) RV Apical Clot
|

|
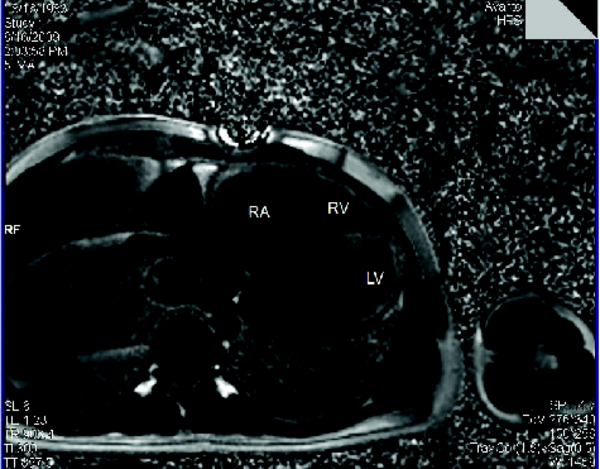
Figure 2.
Cardiac MRI: Displacement of Thickened Septal Tricuspid Valve Leaflet toward RV
|

|
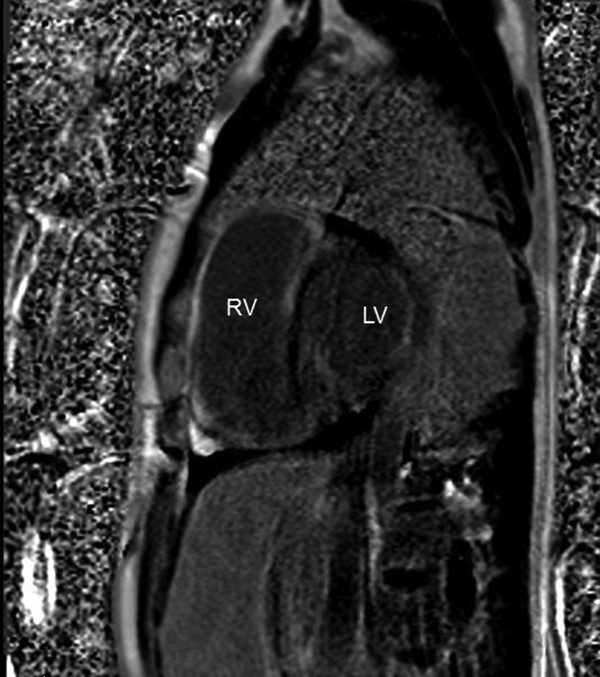
Figure 3.
Cardiac MRI: An Extensive Intramyocardial Hyperenhancement of Left Ventricle with Sparing of Sub Endocardium
|

|
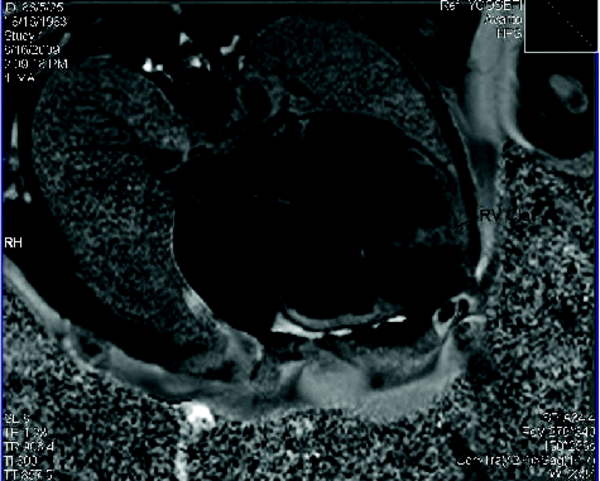
Figure 4.
Cardiac MRI: An Extensive Intramyocardial Hyperenhancement of Left Ventricle with Sparing of Sub Endocardium, Short Axis View
|

|
Figure 5.
Cardiac MRI: Hyper Enhancement of Right Ventricle, Right Atrium and Inter Atrial Wall and a Clot in Right Ventricle
|
3. Discussion
Patients who clinically present with right-sided cardiac enlargement may have dysplasia of the tricuspid valve, an unguarded tricuspid orifice, tricuspid valve prolapse, arrhythmogenic right ventricular dysplasia, Uhl anomaly or parchment right ventricle, trauma, endocarditis, or dilatation of the tricuspid valve annulus secondary to pulmonary valve regurgitation (1). Acquired causes of tricuspid regurgitation and right-sided cardiac enlargement seen in adults also include carcinoid syndrome, pulmonary hypertension, and left heart failure, though the last two are unlikely to be mistaken for Ebstein’s anomaly on the basis of clinical or radiographic findings (1-4). Precise morphologic characterization is vitally important in patients with Ebstein anomaly. Ebstein’s anomaly is primarily diagnosed by echocardiography. A thorough transthoracic echocardiography may be required to make the diagnosis, assess the severity of the anatomic lesion, and determine the effects on cardiac function (1-8). When available and of high quality, cardiac MRI with contrast-enhanced 3-dimensional (3D) MRA would be able to provide information while echocardiography cannot, as was represented in our patient. CMR can show both anatomy and function reliably, with a very good quality and the pulmonary arteries and tricuspid valve can be evaluated at the same study (1, 6-8). Using CMR volumetric studies and quantitative measures of right heart size and function could be performed more delicately and perhaps more robustly than the echocardiography alone even in the presence of the severe disease and significant distortion in the RV anatomy. Echocardiography and CMR could provide complementary data in evaluation of Ebstein’s anomaly. Although CMR imaging can provide volumetric measures of the right heart reliably and reproducibly, echocardiography would be still the best in the assessment of tricuspid valve morphology and small shunts, however. The posterior tricuspid valve leaflet and tricuspid valve fenestrations are better visualized with CMR. So for visualization of the posterior tricuspid valve leaflet and quantitative assessment of the right ventricular size and function, CMR is preferable (6, 8). For appropriate risk stratification in Ebstein’s anomaly, both CMR and echocardiography should be performed before cardiac surgery (6, 8). In Ebstein’s anomaly, the pathologic changes may not be confined to the right side of the heart. In our patient, LV was severely dysfunctional. LV dysfunction for patients with Ebstein’s anomaly has been related to the paradoxical septum motion, age, mitral valve disease, and rarely to myocardial infarction. Additional abnormalities of the LV cavity and contour have been described (1, 4). Regional abnormalities of LV contraction occur in up to 67% of patients with hypokinesis, dyskinesis, diastolic bulging, and premature diastolic distension especially of the septum or anterobasal myocardium. Increased fibrosis unrelated to age has also been described (2, 5). In Ebstein’s anomaly, the pathology of the LV myocardium has not been clearly delineated. Monibi et al., using LV angiography, reported that some patients with Ebstein’s malformation have abnormalities of the left side including mitral valve prolapse, LV dysfunction, or both. In nine of 13 patients in the series of Monibi et al. the LV showed contour abnormalities with an unusually elongated and distorted long axis and irregularity of the septal and lateral walls. Of the 13 patients, 12 showed an abnormal contraction pattern (hypokinesis in nine and dyskinesis in three). Sharma et al. analysed LV angiography in ten patients with Ebstein’s anomaly and noted contour abnormalities in nine of them. Global hypokinesis was present in five of 10 patients in their report (2, 5). The significance of this LV dysfunction may have important clinical and prognostic implications. So far, diminished exercise capacity for patients with Ebstein’s anomaly has been attributed mostly to right-sided heart problems and right-to-left shunting in the presence of ASDs (2, 5). As in our patient, structural and functional alterations of the LV may also play a role to diminish exercise capacity. In conclusion, LV dysfunction may be found with Ebstein’s anomaly with different pathophysiologies and CMR could serve as a non-invasive study to discover the most relevant causes of myocardial damage. However, the clinical significance of these CMR parameters has yet to be determined.
Footnotes
References
- 1. Gates J. Ebstein Anomaly. 2008; [Mar 6, 2023]; Available from: emedicine.medscape.com
- 2. Attenhofer Jost CH, Connolly HM, Warnes CA, O'Leary P, Tajik AJ, Pellikka PA, et al. Noncompacted myocardium in Ebstein's anomaly: initial description in three patients. J Am Soc Echocardiogr. 2004;17(6):677-80. [DOI] [PubMed]
- 3. Bai W, Tang H, An Q, Wu J. An unusual malformation of tricuspid valve. J Am Soc Echocardiogr. 2008;21(4):407 e3-4. [DOI] [PubMed]
- 4. Marcu CB, Donohue TJ. A young man with palpitations and Ebstein's anomaly of the tricuspid valve. CMAJ. 2005;172(12):1553-4. [DOI] [PubMed]
- 5. Attenhofer Jost CH, Connolly HM, O'Leary PW, Warnes CA, Tajik AJ, Seward JB. Left heart lesions in patients with Ebstein anomaly. Mayo Clin Proc. 2005;80(3):361-8. [PubMed]
- 6. Attenhofer Jost CH, Edmister WD, Julsrud PR, Dearani JA, Savas Tepe M, Warnes CA, et al. Prospective comparison of echocardiography versus cardiac magnetic resonance imaging in patients with Ebstein's anomaly. Int J Cardiovasc Imaging. 2012;28(5):1147-59. [DOI] [PubMed]
- 7. Palmerini E, Federici D, Del Pasqua A, Bernazzali S, Lisi M, Chiavarelli M, et al. Echocardiographic Assessment of Ebstein's Anomaly in a 60-Year-Old Man. Case Rep Med. 2009;2009:653741. [DOI] [PubMed]
- 8. Yalonetsky S, Tobler D, Greutmann M, Crean AM, Wintersperger BJ, Nguyen ET, et al. Cardiac magnetic resonance imaging and the assessment of ebstein anomaly in adults. Am J Cardiol. 2011;107(5):767-73. [DOI] [PubMed]
")


