 Home
Home Archive
Archive Search
Search Sign In
Sign In Site Menu
Site Menu


This Article

Citations
 CrossRef (0)
CrossRef (0) - Google Scholar
-
Scopus (0)

Except where otherwise noted, this work is licensed under Creative Commons Attribution-NonCommercial 4.0 International License.
Interesting Images 2
Keywords: Dyspnea, Pulmonary hypertension, Chest Computed Tomographic Scan
1. Introduction
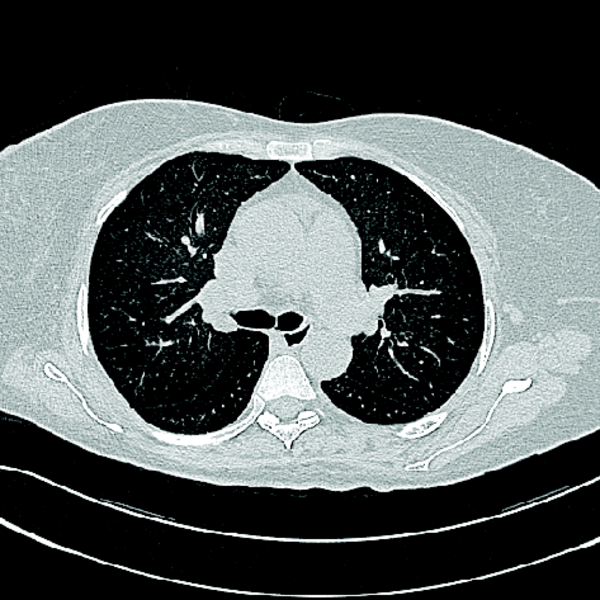
A 57 year –old- woman presented with recent exacerbation of dyspnea on exertion, New York Heart Association (NYHA) functional class III-IV. Physical examination revealed arterial O2 desaturation about 85% at room air associated with Ascites and peripheral edema. Transthoracic echocardiography showed significant pulmonary arterial hypertension about 85 mmHg besides normal LV systolic function (EF=55%) . Right heart catheterization was done and hemodynamic study showed PAP=80/35 mmHg, PCWP=12 mmHg. Cardiovascular CT images are as the following.
Based on the CT images what is the diagnosis?

|
Figure 1a
Cardiovascular CT images
|

|
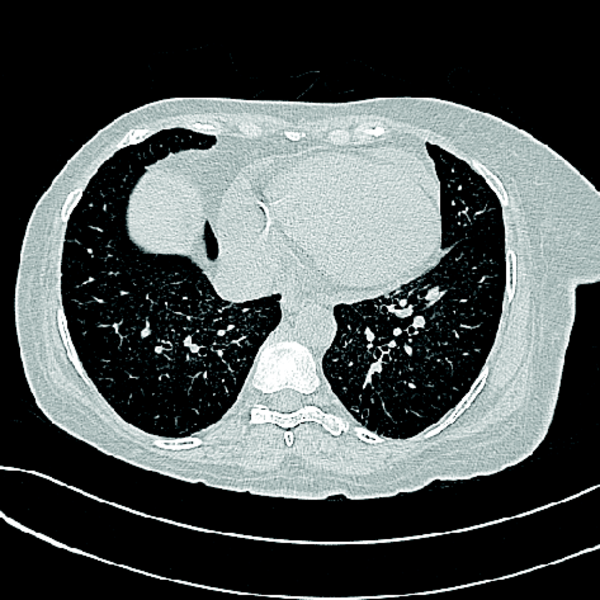
Figure1 b
Cardiovascular CT images
|

|
Figure 1c
Cardiovascular CT images
|
Answer: Pulmonary artery enlargement associated with centrilobular ground glass opacities and increased interstitial pattern , few small mediastinal lymph nodes,pericardial effusion all together are in favor of pulmonary arterial hypertension and pulmonary veno-occlusive disease (PVOD). According to these features PVOD should be considered.
Editorial comment:Pulmonary veno-occlusive disease (PVOD) is a rare form of pulmonary arterial hypertension (PAH) with very poor prognosis. A diffuse fibrous intimal proliferation that predominantly affects the post-capillary venous pulmonary vessels, venules and small veins is the PVOD histopathological hallmark. A noninvasive approach using high-resolution computed tomography of the chest, arterial blood gas analyses, pulmonary function tests and bronchoalveolar lavage could be helpful for the detection of PVOD(1). In patients with PVOD, axial CT image (lung window) shows geographic ground-glass densities, extensive septal thickening and fibrosis, enlarged peripheral pulmonary arteries(2).In these patients, ground-glass attenuation is thought to be secondary to alveolar edema and hemorrhage from venous occlusion.
Footnotes
References
- 1. Pe-a E , Dennie C , Veinot J , Hernández Mu-iz S. Pulmonary Hypertension: How the Radiologist Can Help Radiographics 2012;32:9-32. [DOI] [PubMed]
- 2. Huertas A , Girerd B , Dorfmuller P, O'Callaghan D , Humbert M , Montani D. Pulmonary Veno-occlusive Disease: Advances in Clinical Management and Treatments Expert Rev Respir Med 2011 Apr;5(2):217-29. [DOI] [PubMed]

")


