 Home
Home Archive
Archive Search
Search Sign In
Sign In Site Menu
Site Menu


This Article

Citations
 CrossRef (0)
CrossRef (0) - Google Scholar
-
Scopus (0)

Except where otherwise noted, this work is licensed under Creative Commons Attribution-NonCommercial 4.0 International License.
Echocardiographic Assessment of the Vibratory Innocent Murmur in Children: a Case-Control Study
Abstract
Background: Vibratory innocent murmur is the most common precordial innocent murmur in children. The mechanism of vibratory innocent murmur is still unclear.
Objectives: The aim of this study is to learn the mechanism of the vibratory innocent murmur.
Patients and Methods: The prospective cross-sectional study was conducted using 32 children who had the vibratory innocent murmur (cases) in Chiang Mai University Hospital and 27 normal healthy children (controls). Two-dimension, Doppler, and tissue Doppler echocardiography were performed on each subject to examine the difference between cases and controls.
Results: The left ventricular false tendon was present in 84% of cases and 22% of controls (P < 0.001). Left ventricular outflow tract velocity was significantly higher in cases than in controls (P < 0.001). Early diastolic myocardial velocity at the base of the interventricular septum was lower in cases with false tendon than those without false tendon (P = 0.048). No significant difference was found regarding ascending aorta diameter, cardiac output and ejection fraction between the two groups. Left ventricular diastolic function was normal in all cases and controls.
Conclusions: The vibratory innocent murmur is associated with the presence of left ventricular false tendon and higher left ventricular outflow tract velocity. The presence of the left ventricular false tendon was somewhat associated with decreased early diastolic myocardial velocity. Normal left ventricular systolic and diastolic function can be used as a reassurance in cases with the vibratory innocent murmur.
Keywords: Echocardiography, Doppler; Heart Murmurs
1. Background
Vibratory innocent heart murmur is the most common precordial innocent murmur in children and is characterized by groaning, vibratory and musical harmonic qualities at the left lower sternal border (1, 2). Prevalence of a grade I - III/VI vibratory innocent murmur is 41% in children in the age group 5 - 14 years (3). The genesis of vibratory innocent murmur is still unclear. In the previous studies of pulse, continuous wave Doppler and color flow echocardiographic assessment, high blood flow velocity in the left ventricular outflow tract (LVOT) and ascending aorta (2-6), increased cardiac output (2, 5), relatively smaller ascending aorta (3, 6, 7), and left ventricular false tendon (8-12) were purported to be responsible for the mechanism of the vibratory innocent murmur. Also, the previous study showed that a musical innocent murmur resulted from a vibration of the cardiac structure (13). Because of the association between peak murmur frequency and systolic left ventricular dimension, the vibratory innocent murmur is thought to originate from the left ventricle (7). New echocardiographic techniques may be showing promise in their ability to identify the early changes of the mechanics of the left ventricle. Tissue Doppler imaging has been recently used as a relatively load-independent measure of suspected early myocardial dysfunction (14). Tissue Doppler echocardiography can measure a regional myocardial velocity for assessment of systolic and diastolic function (15).
2. Objectives
To the best of our knowledge, there is no previous study of tissue Doppler imaging of the vibratory innocent murmur. Therefore, the objective of this study is to evaluate the mechanism of the vibratory innocent murmur and the left ventricular function using conventional and tissue Doppler echocardiography.
3. Patients and Methods
We prospectively studied 32 children who had been identified as having vibratory innocent murmur by the clinical assessment of the musical harmonic qualities at the left lower sternal border and 27 normal healthy children without murmur in Chiang Mai University Hospital. Patients with fever, anemia and congenital heart disease were excluded. Two-dimension, pulse wave and continuous wave Doppler, and tissue Doppler echocardiography were performed. The study protocol was approved by the Chiang Mai University Review Board. All children and parents had completed consent forms.
3.1. Doppler Echocardiography
Doppler echocardiographic evaluation was performed using the Philips Sonos 7500. Two-dimension echocardiography was performed to assess the possible presence of the left ventricular false tendon, and also the dimensions of the LVOT, aortic root and ascending aorta. Pulse wave Doppler at mitral valve and pulmonary vein, and tissue Doppler imaging were performed to evaluate left ventricular diastolic function. Pulse wave Doppler of mitral valve flow indicated peak early ventricular filling velocity (E), peak atrial contraction velocity (A), A-wave duration and deceleration time. Pulse wave Doppler of pulmonary venous flow included systolic forward flow velocity, diastolic forward flow velocity, atrial reversal flow velocity and atrial reversal flow duration. Tissue Doppler imaging signals were obtained from an apical four-chamber view at the interventricular septum and left ventricular free wall. Tissue Doppler imaging variables included systolic myocardial velocity (Sm), early diastolic myocardial velocity (Em), late diastolic myocardial velocity (Am) and isovolumic relaxation time. Echocardiographic data also included LVOT velocity, left ventricular ejection fraction and cardiac output. Left ventricular diastolic dysfunction was graded using pulse wave Doppler of mitral and pulmonary venous flows and tissue Doppler imaging (16, 17).
3.2. Statistical Analysis
All statistical calculations were assessed using commercially available software (SPSS Version 16, SPSS Inc., Chicago, IL). Continuous data are expressed as median and range. Categorical data are summarized with the number and percentage. Comparison of pulse wave Doppler and tissue Doppler parameters between the two groups was performed using a t-test, Wilcoxon rank sum as appropriate. Multivariate analysis was performed for predictors of the innocent murmur. A P value < 0.05 was considered statistically significant.
4. Results
Thirty-two children with the vibratory innocent murmur in Chiang Mai University Hospital and 27 normal healthy children were studied. Median age of cases and controls was 39.7 months (4.3 - 175.3) and 42.6 months (9.4 – 87.7), respectively. Fourteen of 32 cases (44%) and 13 of 27 controls (48%) were female. Heart rate, blood pressure and body surface area were not significantly different between the two groups. Left ventricular false tendon was present in 84% of cases and 22% of controls (P < 0.001) (Table 1). LVOT velocity was significantly higher in cases than in controls (P < 0.001). Aortic root diameter was smaller in cases than the controls (P = 0.02). Peak early ventricular filling velocity (E) and peak atrial contraction velocity (A) of mitral valve flow were significantly higher in cases with innocent murmur than those of the controls (P = 0.02 and P = 0.002, respectively) (Table 2). No significant difference was found regarding pulmonary vein flow velocity, left ventricular out flow tract diameter, ascending aorta diameter, cardiac output and left ventricular ejection fraction between the two groups. For the multivariate analysis, the left ventricular false tendon and LVOT velocity were demonstrated to be the independent predictors for the presence of the innocent murmur (P = 0.0011 and P = 0.0004, respectively).
|
|
Table 1.
Comparison of Two-Dimensional and Doppler Echocardiography Between Cases With Vibratory Innocent Murmur and the Controls a,b
|
|
|
Table 2.
Comparison of Pulse Wave Doppler of Mitral Valve Flow and Pulmonary Vein Flow Between Cases With Vibratory Innocent Murmur and the Controls a
|
4.1. Tissue Doppler Echocardiography
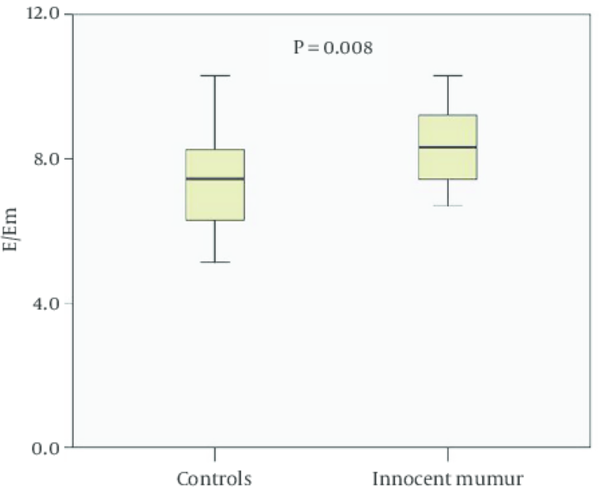
Systolic myocardial velocity, early diastolic myocardial velocity, late diastolic myocardial velocity, and isovolumic relaxation time at the basal, mid and apex parts of the interventricular septum and left ventricular free wall were not significantly different between cases and the controls. However, the ratio of early ventricular filling velocity to early diastolic myocardial velocity (E/Em) at the base of the interventricular septum was higher in cases with innocent murmur than the controls (P = 0.008) (Figure 1). Left ventricular diastolic function graded by using pulse wave Doppler of mitral and pulmonary vein flow and tissue Doppler imaging was normal in all cases and controls.

|
Figure 1.
Graphic Display Comparing the Ratio of Early Ventricular Filling Velocity to Early Diastolic Myocardial Velocity (E/Em) at the Basal Level of the Interventricular Septum Between Cases With Innocent Murmur (N = 32) and Controls (N = 27)
|
4.2. The Presence of Left Ventricular False Tendon
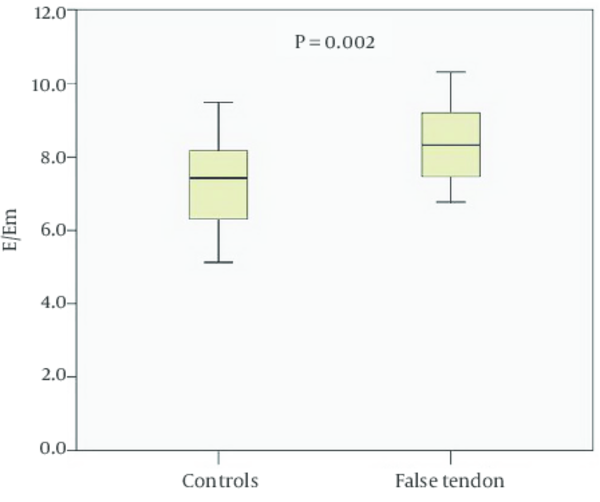
The presence of left ventricular false tendon was analyzed in both cases with innocent murmur and the controls. Early diastolic myocardial velocity (Em) at the base of the interventricular septum was lower in cases with false tendon than those without false tendon (P = 0.048). The ratio of early ventricular filling velocity to early diastolic myocardial velocity (E/Em) at the base of the interventricular septum (Figure 2) and LVOT velocity was significantly higher in cases with false tendon than those without false tendon (P = 0.002 and P = 0.0034, respectively). Peak early ventricular filling velocity of mitral valve flow, pulmonary vein flow velocity, cardiac output, and left ventricular ejection fraction were not significantly different between the two groups.

|
Figure 2.
Graphic Display Comparing the Ratio of Early Ventricular Filling Velocity to Early Diastolic Myocardial Velocity (E/Em) at the Basal Level of the Interventricular Septum Between Cases With Left Ventricular False Tendon (N = 33) and Those Without False Tendon (N = 26)
|
5. Discussion
The present study shows that the mechanism of the vibratory innocent murmur is associated with the presence of left ventricular false tendon and high blood flow velocity in LVOT. The presence of the left ventricular false tendon was somewhat associated with decreased early diastolic myocardial velocity, increased LVOT velocity, and increased ratio of early ventricular filling velocity to early diastolic myocardial velocity. Although, E/Em predicted left ventricular diastolic pressure, left ventricular diastolic function graded by using pulse wave Doppler of mitral and pulmonary vein flow and tissue Doppler imaging was normal in all cases with the false tendon condition.
Two-dimension, pulse wave Doppler, continuous wave Doppler and color flow echocardiography were used for assessment of the mechanism of the vibratory innocent murmur. High blood flow velocity in the region of the LVOT and ascending aorta, resulting from the larger cardiac output passing through a relatively smaller ascending aorta with a vibratory phenomenon of the aortic valve were the origin of the vibratory innocent murmur (2-7). Kenchaiah et al. and Perry LW, et al. reported that the presence of left ventricular false tendon was associated with the precordial innocent murmur (8, 10). In the present study, high blood flow velocity in LVOT and a vibratory phenomenon of the left ventricular false tendon were proposed as the mechanism of the vibratory innocent murmur.
Tissue Doppler imaging can measure a regional myocardial velocity for assessment of the early myocardial dysfunction (14, 15). To the best of our knowledge, there is no previous study of tissue Doppler echocardiography in the vibratory innocent murmur. In the present study, peak early ventricular filling velocity of mitral valve flow was significantly higher in cases with innocent murmur than those of the controls. Likewise, the ratio of early ventricular filling velocity to early diastolic myocardial velocity (E/Em) at the base of the interventricular septum was significantly higher in cases with innocent murmur than in the controls. Early diastolic myocardial velocity at the base of the interventricular septum was significantly lower than in cases with left ventricular false tendon than those without false tendon. Also, the ratio of early ventricular filling velocity to early diastolic myocardial velocity was significantly higher in cases with false tendon than those without false tendon. It is postulated that left ventricular false tendon may cause the decrease of early diastolic myocardial velocity. However, left ventricular diastolic function graded by using pulse wave Doppler of mitral and pulmonary vein flow and tissue Doppler imaging was normal in both cases with false tendon and those without false tendon.
The vibratory innocent murmur is strongly associated with the presence of left ventricular false tendon and high velocity blood flow in the left ventricular outflow tract. Left ventricular diastolic function is normal in cases with left ventricular false tendon. Normal left ventricular systolic and diastolic function can be used as a reassurance to parents in cases with the vibratory innocent murmur and left ventricular false tendon.
References
- 1. Rosenthal A. How to distinguish between innocent and pathologic murmurs in childhood. Pediatr Clin North Am. 1984;31(6):1229-40. [PubMed]
- 2. Celebi A, Onat T. Echocardiographic study on the origin of the innocent flow murmurs. Pediatr Cardiol. 2006;27(1):19-24. [DOI] [PubMed]
- 3. Van Oort A, Hopman J, De Boo T, Van Der Werf T, Rohmer J, Daniels O. The vibratory innocent heart murmur in schoolchildren: a case-control Doppler echocardiographic study. Pediatr Cardiol. 1994;15(6):275-81. [PubMed]
- 4. Klewer SE, Donnerstein RL, Goldberg SJ. Still's-like innocent murmur can be produced by increasing aortic velocity to a threshold value. Am J Cardiol. 1991;68(8):810-2. [PubMed]
- 5. Gardiner HM, Joffe HS. Genesis of Still's murmurs: a controlled Doppler echocardiographic study. Br Heart J. 1991;66(3):217-20. [PubMed]
- 6. Schwartz ML, Goldberg SJ, Wilson N, Allen HD, Marx GR. Relation of Still's murmur, small aortic diameter and high aortic velocity. Am J Cardiol. 1986;57(15):1344-8. [PubMed]
- 7. Donnerstein RL, Thomsen VS. Hemodynamic and anatomic factors affecting the frequency content of Still's innocent murmur. Am J Cardiol. 1994;74(5):508-10. [PubMed]
- 8. Perry LW, Ruckman RN, Shapiro SR, Kuehl KS, Galioto FJ, Scott L3. Left ventricular false tendons in children: prevalence as detected by 2-dimensional echocardiography and clinical significance. Am J Cardiol. 1983;52(10):1264-6. [PubMed]
- 9. Malouf J, Gharzuddine W, Kutayli F. A reappraisal of the prevalence and clinical importance of left ventricular false tendons in children and adults. Br Heart J. 1986;55(6):587-91. [PubMed]
- 10. Kenchaiah S, Benjamin EJ, Evans JC, Aragam J, Vasan RS. Epidemiology of left ventricular false tendons: clinical correlates in the Framingham Heart Study. J Am Soc Echocardiogr. 2009;22(6):739-45. [DOI] [PubMed]
- 11. Philip S, Cherian KM, Wu MH, Lue HC. Left ventricular false tendons: echocardiographic, morphologic, and histopathologic studies and review of the literature. Pediatr Neonatol. 2011;52(5):279-86. [DOI] [PubMed]
- 12. Silbiger JJ. Left ventricular false tendons: anatomic, echocardiographic, and pathophysiologic insights. J Am Soc Echocardiogr. 2013;26(6):582-8. [DOI] [PubMed]
- 13. Stein P, Sabbah H, Lakier J. Origin and clinical relevance of musical murmurs. International Journal of Cardiology. 1983;4(1):103-12. [DOI]
- 14. Eidem BW, McMahon CJ, Ayres NA, Kovalchin JP, Denfield SW, Altman CA, et al. Impact of chronic left ventricular preload and afterload on Doppler tissue imaging velocities: a study in congenital heart disease. J Am Soc Echocardiogr. 2005;18(8):830-8. [DOI] [PubMed]
- 15. Border WL, Michelfelder EC, Glascock BJ, Witt SA, Spicer RL, Beekman R3, et al. Color M-mode and Doppler tissue evaluation of diastolic function in children: simultaneous correlation with invasive indices. J Am Soc Echocardiogr. 2003;16(9):988-94. [DOI] [PubMed]
- 16. Nagueh SF, Appleton CP, Gillebert TC, Marino PN, Oh JK, Smiseth OA, et al. Recommendations for the evaluation of left ventricular diastolic function by echocardiography. Eur J Echocardiogr. 2009;10(2):165-93. [DOI] [PubMed]
- 17. Dragulescu A, Mertens LL. Developments in echocardiographic techniques for the evaluation of ventricular function in children. Arch Cardiovasc Dis. 2010;103(11-12):603-14. [DOI] [PubMed]
")


