 Home
Home Archive
Archive Search
Search Sign In
Sign In Site Menu
Site Menu


This Article

Citations
 CrossRef (0)
CrossRef (0) - Google Scholar
-
Scopus (0)

Except where otherwise noted, this work is licensed under Creative Commons Attribution-NonCommercial 4.0 International License.
Echocardiographic Evaluation of Effects of Different Training Regimens on Left Ventricle Structure and Function in Female Athletes
Abstract
Background: Professional training regimens are accompanied with morphologic alteration and cardiac function which is known as “athlete’s heart” which is defined by left ventricular hypertrophy and other echocardiographic features.
Objectives: The present study aims to evaluate the effect of different training protocols such as endurance-training, strength training protocols and concurrent protocols on heart structures.
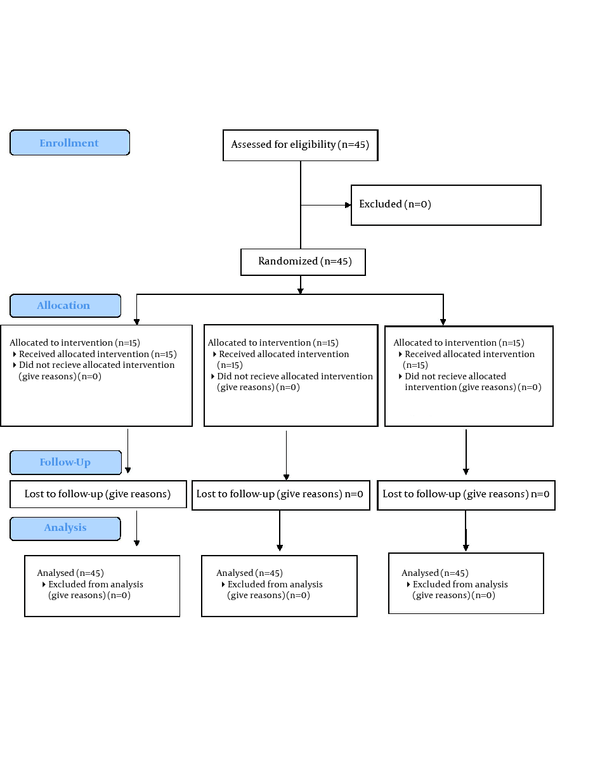
Patients and Methods: Forty five young female volunteer athletes were included and received different training regimens (endurance-training, strength training and concurrent groups) for a 10 week period as study intervention. Standard color Doppler echocardiography was performed for assessment of the left ventricular activity.
Results: As a result, 45 athletes ended the study training regimens. Mean of cardiac parameters was not significantly different among athletes under study before the beginning of the study training regiments. Mean of end diastolic diameter among athletes of strength-trained group had been significantly increased after receiving the study training regiments. Mean of posterior wall thickness had been significantly increased in athletes of strength and concurrent groups. Mean of posterior wall thickness had been decreased in athletes of endurance-training group. Mean of heart rate was significantly decreased among the athletes of endurance-training and concurrent-training groups.
Conclusion: The combination of both endurance-training and strength training protocols caused largest increases in left ventricular internal dimension and left ventricular wall thickness among the trial participants.
Keywords: Athlete Heart; Echocardiography; Sports
1. Introduction
Regular, hard and professional training regimens are accompanied with morphologic alteration and cardiac function which is known as “athlete’s heart”. (1-4). Athlete's heart is usually an incidental finding during a routine screening or during tests for other medical issues. An enlarged heart can be seen at echocardiography or sometimes on a chest X-ray. Left ventricular hypertrophy is less than 13 mm and left ventricular end diastolic diameter is less than 60mm.It’s been shown that cardiac alterations like bradycardia, left ventricular hypertrophy and stroke volume increase may be seen in athletes who exercise for long times (5). Some cardiac characters such as wall thickness and dimensions of left ventricle chamber might be participating in this adaptation. Different training specifications such as pressure or volume overload can cause several changes in morphological heart features (6). Several echocardiography studies accomplished on athletic or non- athletic ones reveal that individuals doing dynamic exercises- like short or long distance- foot- race runners will catch ventricular dimension enlargement. on the the other hand, athletes of static or resistance sports seem to have thicker ventricular walls and left ventricle dimensions which increase a little or normal (7). Presumably, echocardiography must be the best non-invasive way which can investigate left ventricular hypertrophy. Attained findings of echocardiography about left ventricle dimensions and sizes are closely accordant with attained findings of left ventricle ventricolography and biopsy (8). Investigations in elite athlete’s heart have recently provided relevant information on the myocardial “reserve” of the left ventricle (LV) (9-13). However, myocardial adaptation to regular training in Iranian female athletes has not been studied so far and very little information about the left ventricle echocardiographic parameters in female athletes are available.
2. Objectives
The present study was designed to assess the role of training in heart features in some volunteers’ female athletes.
3. Patients and Methods
The present study was performed by parallel design in one blinded control trial study with 15 participants in each studied group. The study was approved by ethical committee of Baqiatallah University of Medical Sciences. Forty five young female volunteer athletes (mean age 21 ± 1.87 yrs.) included in the present study. Exclusion criteria include the evidence of cardiovascular and metabolic diseases in patients whose presence had been confirmed by the clinical history. Although it is not a mandatory exam in order to obtain the eligibility, all subjects underwent an echocardiographic exam at rest. Study participants received different training regimens for a 10 week period. Warm up period: includes running for 10 minutes with 40-45% of MHR before beginning the exercise. -In the first and second week: running for 2x10 minutes for 60-65% of maximum heart rate (MHR). -In the third and fourth week: running for 2x12 minutes for 60-65% of MHR. -In the fifth and sixth week: running for 2x13 minutes for 70-75% MHR. -In the seventh and eighth week: running for 2x14 minutes for 70-75% MHR. -In the ninth and tenth week: running for 2x15 minutes for 75-80% MHR. The sports that were done: press (chest, foot), sitting and lying and standing on toe. These sports were done for two sessions a week for 10 weeks. They were done consecutively with 2-3 minutes rest interval and, the rest interval was 60-90 seconds after each. In the fourth and eighth week the load decreased for preventing from overraining. About half of exercises of each group were done in each session. But strength sports were done at first. All the trainings were done for two times a week. Standard color Doppler echocardiography was done by vivid 3 (GE) and probe 3MHz. The images were obtained from the left lateral decubitus. All the measurements were the average of three to five cardiac cycles. M-mode measurements were done in parasternal long axis view, Doppler and tissue Doppler studies were done in apical 4-chamber, 2-chamber and 3-chamber views. For standard diastolic Doppler mitral inflow, images were obtained from apical 4-chamber view and (E and A peak velocities (m/s) and E/A ratio, deceleration time DT (ms). Forty five young female volunteer athletes participated in the study (mean age 21 ± 1.87 years.). Trial participants were randomly selected and allocated into the trial groups. Present trial was blinded trial study and cardiologist who performed echocardiographic examination, was blinded for training regimens which passes by trial participants. Qualitative variables were presented with number and frequency and quantitative variables were presented with mean and standard deviation. Chi-square test and analysis of variance were used for comparing qualitative and quantitative variables among the trial groups. All Pvalues ≤0.05 were assumed as significant results.3.1. Trial Design
3.2. Participants
3.3. Interventions
3.3.1. A-The training protocol for endurance-trained group (E) was as follow:
3.3.2. B-The training protocol for strength-trained group (S) was as follow:
3.3.3. C-The training protocol for concurrent group (C) was as follow:
3.4. Outcomes
3.4.1. Sample Size
3.4.2. Randomization
3.4.3. Blinding
3.5. Statistical Analysis
4. Results
Finally 45 athletes ended the study training regimens. Mean of age among athletes was not significantly different among the study groups (P = 0.09). Mean of cardiac parameters was not significantly different among the athletes before beginning the study training regimens (Table 1) (Figure 1). Trial participants were equally and randomly allocated to three trial groups (each group 15 persons). Although mean of intraventricular diameters among study participants was increased after study regimens, athletes of endurance training regimen had significant increase. Mean of end diastolic diameter among athletes of strength-trained group had been significantly increased after receiving study training regiments. Mean of posterior wall thickness had been significantly increased in athletes of strength (P = 0.01) and concurrent groups (P = 0.00). Mean of posterior wall thickness had been decreased in athletes of endurance-training group. Mean of heart rate was significantly decreased among athletes of endurance-training (P = 0.03) and concurrent-training groups (P = 0.00).4.1. Study Participants
4.2. Baseline Data

![]()
4.3. Number Analyzed
4.4. Outcomes
![]()
5. Discussion
Based upon the findings from the present study, the mean of intra ventricular diameters and heart rate had been significantly changed among athletes of endurance-training regimen after beginning the training regimens. Previous studies reported the high prevalence of LV dilation among endurance-trained athletes (7, 14). DuManoir et al. recently reported significant increases in resting LV cavity dimensions, stroke volume, and mass after 10 week of a three time- rowing sessions in a week (15). The increase in left ventricle mass is correlated tightly with the increase in LV end-diastolic volume but not with changes in wall thickness. Although LV stroke volume was increased following training, resting cardiac output, due to a marked reduction in resting heart rate, was significantly reduced. This finding deserves further study. In addition, Endurance athletes experienced significant increase in LV diastolic tissue velocities, which were positively correlated with the magnitude of LV mass increase. In aggregate, our data suggest that endurance training produces LV dilation with accompanying augmentation of LV diastolic function. Adaptation of heart to endurance training with an increase in both diameter and wall thickness is useful if we take into account the heart rate and blood pressure responses during intense exercise (2). The cardiac output of trained endurance athletes may increase from 5 to 6 L/min at rest to up to 40 L/min during maximal exercise (16). The heart adapts to this volume load with an increase in internal diameter. Blood pressure also increases during endurance exercise, although to a lesser extent than during strength training. Blood pressure readings of 69/175 mm Hg during treadmill running were recorded by Palatini et al(17). In other words, pure volume load during endurance training does not exist; during long distance running, the heart has to adapt to volume and pressure load, whereby the endurance-trained heart shows an increase in both left ventricular internal diameter and left ventricular wall thickness. In athletes of endurance-training regimen, only end diastolic diameters and posterior wall thickness had been significantly changed during strength-training. Exposing heart tostrength training with a slight strength in left ventricular internal diameter and a large increase in left ventricular wall thickness can be explained on the basis of blood pressure response and cardiac output during weight lifting (18-21). During the heavy-resistance exercise, arterial blood pressure shows a large increase, (near to 350-480 mm Hg (19). However, heart rate and cardiac output do not remain unchanged but show an increase during strength training. MacDougall et al. demonstrated that during weight lifting, heart rate ranged from 102 bpm, between sets, to peak values of 170 bpm Accordingly, pure pressure load during strength training does not exist (19). In athletes who had concurrent endurance and strength-training regimen, only posterior wall thickness and heart rate had been significant changed during strength-training. Rowing and cycling represent typical strength and endurance sports like combined dynamic and static exercise of large groups of muscles. Top-level cyclists can perform with a near-maximal heart rate for long periods of time, sometimes up to six hours. Systolic and mean arterial blood pressures also increases during cycling; Systolic blood pressure might increase to 200 mm Hg during maximal exercise testing on the bicycle ergometer (21, 22). During rowing, heart rate increases to near-maximal values of '190 bpm, with peak systolic blood pressure waves of '200 mm Hg (23). The combination of both extreme volume load and extreme pressure load may explain why the high increases in left ventricular internal dimension and left ventricular wall thickness are found in cyclists and rowers.
Acknowledgments
We appreciate the help of Miss Sharifi
Footnotes
References
- 1. Maron BJ. Structural features of the athlete heart as defined by echocardiography. J Am Coll Cardiol. 1986;7(1):190-203. [PubMed]
- 2. Pluim BM, Zwinderman AH, van der Laarse A, van der Wall EE. The athlete's heart. A meta-analysis of cardiac structure and function. Circulation. 2000;101(3):336-44. [PubMed]
- 3. Rawlins J, Bhan A, Sharma S. Left ventricular hypertrophy in athletes. Eur J Echocardiogr. 2009;10(3):350-6. [DOI] [PubMed]
- 4. Shephard RJ. The athlete's heart: is big beautiful? Br J Sports Med. 1996;30(1):5-10. [PubMed]
- 5. Spirito P, Pelliccia A, Proschan MA, Granata M, Spataro A, Bellone P, et al. Morphology of the "athlete's heart" assessed by echocardiography in 947 elite athletes representing 27 sports. Am J Cardiol. 1994;74(8):802-6. [PubMed]
- 6. Mitchell JH, Haskell W, Snell P, Van Camp SP. Task Force 8: classification of sports. J Am Coll Cardiol. 2005;45(8):1364-7. [DOI] [PubMed]
- 7. Pelliccia A, Culasso F, Di Paolo FM, Maron BJ. Physiologic left ventricular cavity dilatation in elite athletes. Ann Intern Med. 1999;130(1):23-31. [PubMed]
- 8. Abernethy WB, Choo JK, Hutter AM, Jr. Echocardiographic characteristics of professional football players. J Am Coll Cardiol. 2003;41(2):280-4. [PubMed]
- 9. Akagawa E, Murata K, Tanaka N, Yamada H, Miura T, Kunichika H, et al. Augmentation of left ventricular apical endocardial rotation with inotropic stimulation contributes to increased left ventricular torsion and radial strain in normal subjects: quantitative assessment utilizing a novel automated tissue tracking technique. Circ J. 2007;71(5):661-8. [PubMed]
- 10. Goffinet C, Chenot F, Robert A, Pouleur AC, le Polain de Waroux JB, Vancrayenest D, et al. Assessment of subendocardial vs. subepicardial left ventricular rotation and twist using two-dimensional speckle tracking echocardiography: comparison with tagged cardiac magnetic resonance. Eur Heart J. 2009;30(5):608-17. [DOI] [PubMed]
- 11. Stanton T, Leano R, Marwick TH. Prediction of all-cause mortality from global longitudinal speckle strain: comparison with ejection fraction and wall motion scoring. Circ Cardiovasc Imaging. 2009;2(5):356-64. [DOI] [PubMed]
- 12. Stefani L, Pedrizzetti G, De Luca A, Mercuri R, Innocenti G, Galanti G. Real-time evaluation of longitudinal peak systolic strain (speckle tracking measurement) in left and right ventricles of athletes. Cardiovasc Ultrasound. 2009;7:17. [DOI] [PubMed]
- 13. Stefani L, Toncelli L, Di Tante V, Vono MC, Cappelli B, Pedrizzetti G, et al. Supernormal functional reserve of apical segments in elite soccer players: an ultrasound speckle tracking handgrip stress study. Cardiovasc Ultrasound. 2008;6:14. [DOI] [PubMed]
- 14. Morganroth J, Maron BJ, Henry WL, Epstein SE. Comparative left ventricular dimensions in trained athletes. Ann Intern Med. 1975;82(4):521-4. [PubMed]
- 15. duManoir GR, Haykowsky MJ, Syrotuik DG, Taylor DA, Bell GJ. The effect of high-intensity rowing and combined strength and endurance training on left ventricular systolic function and morphology. Int J Sports Med. 2007;28(6):488-94. [DOI] [PubMed]
- 16. Ekblom B, Hermansen L. Cardiac output in athletes. J Appl Physiol. 1968;25(5):619-25. [PubMed]
- 17. Palatini P, Mos L, Di Marco A, Mormino P, Munari L, Del Torre M. Intra-arterial blood pressure recording during sports activities. Journal of hypertension. 1987;5:479-81.
- 18. MacDougall JD, McKelvie RS, Moroz DE, Sale DG, McCartney N, Buick F. Factors affecting blood pressure during heavy weight lifting and static contractions. J Appl Physiol. 1992;73(4):1590-7. [PubMed]
- 19. MacDougall JD, Tuxen D, Sale DG, Moroz JR, Sutton JR. Arterial blood pressure response to heavy resistance exercise. J Appl Physiol. 1985;58(3):785-90. [PubMed]
- 20. Perez-Gonzalez JE. Factors determining the blood pressure responses to isometric exercise. Circ Res. 1981;48(6 Pt 2):I76-86. [PubMed]
- 21. Vitcenda M, Hanson P, Folts J, Besozzi M. Impairment of left ventricular function during maximal isometric dead lifting. J Appl Physiol. 1990;69(6):2062-6. [PubMed]
- 22. Mitchell JH, Haskell WL, Raven PB. Classification of sports. J Am Coll Cardiol. 1994;24(4):864-6. [PubMed]
- 23. Clifford PS, Hanel B, Secher NH. Arterial blood pressure response to rowing. Med Sci Sports Exerc. 1994;26(6):715-9. [PubMed]
")


